
Effectiveness of intensive short-term psychodynamic psychotherapy on reduced death anxiety, depression and feeling of loneliness among women with breast cancer
Mahdavi Abed1*, Jenaabadi Hossein2, Sepehryeganeh Shahrbanoo3, Gholamali Lavasani Masoud4, Mansoureh Hajhosseini5
1 Department of Psychology, Faculty of Psychology and Educational, University of Tehran, Tehran, Iran. 2 Professor of Psychology, Department of Psychology, Faculty of Psychology and Educational Sciences, University of Sistan and Baluchestan, Tehran, Iran. 3 Department of Psychology, Faculty of Psychology and Educational Sciences, University of Islamic Azad, Karaj Branch, Iran. 4 Associate Professor, Faculty of Psychology and Educational, University of Tehran, Tehran, Iran. 5Assistant Professor, Faculty of Psychology and Educational, University of Tehran, Tehran, Iran.
Correspondence: Mahdavi Abed, Department of Psychology, Faculty of Psychology and Educational, University of Tehran, Tehran, Iran. Email: [email protected].
|
ABSTRACT Background: Although cancer causes numerous psychological complications, it has recently been determined that psychological pressures have a profound effect on accelerating the progression and growth of various types of malignant tumors, without creating and generating them. The present study was conducted to investigate the effectiveness of intensive short-term psychodynamic psychotherapy on reduced death anxiety, depression and feeling of loneliness among women with breast cancer. Method: The research method used was a single subject design with a case study with a two-month follow-up in women referred to health centers in Tehran. Of the women, 4 people, with psychological problems, who were volunteered for treatment, were selected through purposeful sampling. The purpose of this sampling method was to select people who were appropriate for the purpose of the study. These people participated in 12 sessions of treatment sessions. The participants participated in 12 treatment sessions. The treatment was carried out according to Davanloo’s intensive short-term pschodynamic psychotherapy. This therapeutic model focuses on clarifying and challenging the defences, experiencing the emotions, and solving intra-psychological conflicts. Templer Death Anxiety Scale, Beck Depression Inventory, and Shortened version of the social and emotional loneliness scale for Adults scales were used in this study and data analysis was conducted using t-test and repeated measures ANOVA. Results: The findings of this study showed that after therapeutic intervention, the amount of death, depression and feelings of loneliness decreased. And, this status remained stable for two months after the end of the sessions, and none of them returned to the previous situation. Conclusions: Therefore, it can be concluded that the implementation of ISTDP has been effective in reducing the psychological problems of the patients. Keywords: Intensive short-term psychodynamic psychotherapy (ISTDP), Death anxiety, Depression, Feeling of loneliness, Breast cancer |
Introduction
According to global statistics, breast cancer is the most commonly diagnosed cancer in women throughout the world [1]. In Iran, breast cancer, with the frequency of 23% of women’s cancer, is the most common cancer in this gender, and in general, 0.87 of the total cause of death in the age group of 15-50 years and 0.99 of the total cause of death in the age group of 69-50 years are related to breast cancer [2]. In western countries, breast cancer is predominantly observed in the subjects over the age of 50, this is while according to studies conducted in our country, the number of cases aged in the range of 40-49 years is more than other age groups [3]. The results of the research indicate that there are obvious consequences of breast cancer such as physical problems (pain and fatigue), psychological problems (anxiety and depression), and other psychosocial problems in patients, which lead to a decrease in quality of life, especially in relation to younger women [4-6]. Breast cancer is one of the diseases that, in addition to physical problems and effects, also has a severe psychological effect in a patient with cancer. In confronting with this disease and diagnosis of cancer, the patient goes through several different psychological stages, and suddenly, the world of woman with a catastrophic cancer collapses, she becomes confused, her small hopes fade against great disappointments and in this situation, no one deeply understands his feelings [7]. Becoming informed of this diagnosis can be very stressful to the patient physically and psychologically, so that it is described as rolling a big stone in a calm sea. Patients experience severe mental and psychological reactions to cancer diagnosis, so that one of the sensations that they face after diagnosing cancer is sense of impending death and being near the death. Today, death anxiety is mentioned as one of the most important psychological components in cancer patients [8, 9]. Among the specific types of anxiety, according to its known source, death anxiety is one of the most important ones. "Death anxiety" is one of the human tensions, which has become more pronounced with the slowing down of population growth rates and aging. Belskey [10] describes death anxiety as the thoughts, fears and emotions associated with the end-of-life and beyond the normal way of life. Death anxiety is defined as an unusual fear of death, accompanied by feelings of fear of death, or anxiety when thinking about the process of dying or what happens after death [11]. Jones et al [12] consider death anxiety as conscious and unconscious fear of death or dying; death anxiety is a complex concept that cannot be easily explained and generally includes concepts of fear of death of self and others. In other words, death anxiety involves the prediction of death of self and the fear of the process of death and dying of the most important people of life, and humans are knowingly aware of their death; however, patients with risky diagnoses such as cancer are inevitably faced with their death [12]. Death anxiety in this group of patients with psychological and even mental disorder can affect their quality of life [12].
Another psychological disorder that has a relatively high prevalence in patients with breast cancer is depression [13]. Depression is a state in which humans feel hard, sad, distressed, and anxious, and feels life bored and dull in the long run. A depressed person does not feel pleased, happy or willing in relation to anything. For depressed people, it is very difficult to start things and they get tired too soon [13]. Studies by Renger and Couter and Bardos Sutherland showed that people with a history of psychological-mental problems, the lack of emotional support from family and friends, the lack of acceptance of physical changes associated with breast cancer and treatment, and the lack of participation in the pleasurable activity, previous history of having a bitter cancer experience in the family, feeling disappointed about the outcome of the treatment, lower age at diagnosis stage and family problems were more susceptible to depression [14]. In addition, feeling of loneliness is one of the psychosocial concerns of cancer patients. Loneliness may be more serious in women with breast cancer, because women are more vulnerable to feelings, and women with this type of cancer are more likely to live longer than other types of cancers [15]. Feeling of loneliness is a distressing and annoying experience that has severe psychological and physical problems [16,17]. Cancer patients who experience loneliness will not only have psychosocial distress, but also will be exposed to more physical hazards with less ability to participate in health behaviors [18]. The symptom of loneliness in the cancer patients is correlated with depression, suicide, anxiety, drug abuse, feeling of misery, and a multiplicity of physical diseases [19,20]. Statistics show that one out of every four people suffers from feeling of loneliness [21]. So far, there have been many psychiatric treatments for people with mental and physical disorders. But one of the new Psychotherapy approaches that is believed to be effective in reducing the psychological problems of women with cancer is intensive short-term dynamic psycho-therapy [22]. Intensive short-term dynamic psycho-therapy is a result of Freud’s Psychoanalysis model developed by Iranian scientist Davanloo at McGill University [22]. In this model, the long-term, low-impact, unorganized and unspecified psycho-analytic method has been turned into a short-term, effective, organized and clear method [22]. In this respect, Malan states that "Freud discovered the subconscious, and Davanloo, how to use it for treatment" [23]. In the view of Malan [24], since discovery of dynamic unconsciousness by Freud, this method has been the greatest advancement in psychotherapy. This therapeutic approach is called dynamic therapy because, like psychoanalysis, relies upon the experience of real feelings, overcoming resistance and exact attention to transition phenomenon. This therapeutic approach is built on the therapeutic relationship and the nature of the disclosure [25]. In this approach, patients are encouraged to regulate their anxiety and change them against their defenses so that they can deal with feelings that they have avoided [26]. Given that cancer creates a serious challenge for people, how to deal with this challenge and how to cope with its consequences, problem solving methods and the provision of correct solutions and how to deal with disorders caused by exposure to this disease are extremely crucial. The psychological consequences of breast cancer and its treatment have been the topic of many research activities. In this regard, intensive short-term psychodynamic psychotherapy (ISTDP) is one of the approaches in psychology that has attracted the attention of researchers and psychologists in recent decades. This approach can help patients to minimize the negative psychological effects of their illness. Strong empirical support for the use of ISTDP for common mental health problems in physical illnesses is fully consistent with the provision of modern health care and emphasis on treatments with empirical support. So far, ISTDP model has been used for a large number of mental disorders and chronic medical illnesses, many of which have been recognized as effective in clinical research. It is worth noting that ISTDP approach is a non-medical treatment that affects not only the components of the disease directly, but also, because of its positive and effective effect on the psychological and emotional factors of patients, can have a significant impact on the promotion of mental health and, consequently, coping with the disease and trying to treat it in patients with breast cancer [27]. Given that the effect of ISTDP approach on certain diseases, including breast cancer, has been scarcely taken into consideration, and pharmaceutical and aggressive therapies have been prioritized. Seemingly, the gap is the impact of ISTDP on the psychological consequences of the disease. Thus, the researcher sought to investigate ISTDP approach affect the psychological components of the patients, such as death anxiety, depression and feeling of loneliness by conducting a short-term psychotherapy course in patients with breast cancer.
Method and Materials
The research method used was a quasi-experimental design with a case study with a two-month follow up in women referred to health centers in Tehran. Of them, 4 people, with psychological problems and criteria for entering into intensive short-term dynamic psycho-therapy, who were volunteered for treatment, were selected through purposeful sampling. The purpose of this sampling method was to select people who were appropriate for the purpose of the study. These people participated in 12 sessions of treatment sessions. The participants participated in 12 treatment sessions. The treatment was carried out according to Davanloo’s intensive short-term dynamic psycho-therapy. This therapeutic model focuses on clarifying and challenging the defences, experiencing the emotions, and solving intra-psychological conflicts. Death anxiety, depression and feeling of loneliness questionnaires were used in this study and data analysis was conducted using t-test and repeated measures ANOVA.
ISTDP model: intensive short-term psychodynamic psychotherapy is a form of short-term psychotherapy that was developed by Professor Habib Davanloo during the period from the 1606's to the 1666's through empirical research and video tapes recorded from patients' treatment sessions. This therapeutic approach includes an exquisite set of therapeutic interventions, each devoted to a specific purpose and goal. This collection is known as "axial dynamics sequence". The therapist examines the patient's current problems at the beginning of the treatment. Having obtained a general understanding of the patient's problems, he/she askes the patient to explain the last instance of his/her problem in order to identify and experience his/her feelings. Pressure to experience feelings is faced with defensive processes and this is the result of the work of therapist the second stage of the therapeutic evaluation. Now the therapist must identify and clarify the defenses. The consequences of defense mechanisms are examined and thus, the treatment enters into a continuous pressure towards the touch of emotions along with the challenge with the aim of avoiding defensive avoidance. The combination of two techniques of pressure and challenge simultaneously creates an intra-psychological conflict in the patient, and leads to the arousal and crystallization of transitional feelings. The therapist, using imagery and imagination to express excited impulses, encourages the patient to express these feelings directly. This process leads to the collapse of the defenses and the extrapolation of the patient's unconscious content and links the pattern of behavior appearing in the transition to its past and present relationships. When a patient's psychological system is opened enough, a cognitive analysis can be undertaken to reinforce the insight from it.
|
Table 1: The Therapeutic Techniques Used in Treatment Sessions to Reduce the Amount of Psychological Problems in Patients with Breast Cancer |
|
Instruments for collecting the data are as follows:
- Templer Death Anxiety Scale (DAS): Templer Death Anxiety Scale [28] contains 15 questions about subjects' attitudes toward death. The subject specifies his/her answer to any question with the choice "Yes or No." Positive answer shows anxiety in the individual. Thus, the scores of this scale can range from zero to fifteen, and a high score indicates a high death anxiety rate in individuals. Templer [28] calculated reliability coefficient of the scale as 0.83. In a study by Rajabi and Bohrani [29], the split-half reliability coefficients of death anxiety scale were calculated as 0.62 after applying Spearman Brown's correction formula.
- Beck Depression Inventory (BDI): The questionnaire consists of 13 self-report items expressing specific symptoms of depression. Each statement of the questionnaire consists of a four-point Likert scale in a range from 0 to 3. The range of its scores is from 0 to 39, which has been developed for the measurement purpose in different areas of symptomology of depression such as emotional, cognitive, motivational and physiological depression. Lightfoot and Oliver [30, 31] reported the Cronbach's alpha coefficient of the shortened form of Beck Depression Inventory (composed of 13 items) as 0.87 and a test-retest reliability of 0.92 within a two-week interval. In a study by Mahdavi et al [32], the reliability of Beck Depression Inventory was calculated using Cronbach's alpha and split-half methods for the whole questionnaire, as 0.94 and 0.90, respectively. This shows that reliability coefficients of the questionnaire are desirable.
- Shortened version of the social and emotional loneliness scale for adults: This scale was designed and developed by Ditommasso, Brannen, and best in [21]. This scale consists of 15 statements and three dimensions, and is scored in a five-point Likert form from completely disagree (1) to completely agree (5). All the statements, except for the statement 14 and 15, are reversely scored. Getting a higher score shows a greater feeling of loneliness in the respective dimension. Cronbach's alpha coefficient of the scale has been reported in the range of .87-.90 [21].
Results
Four women with breast cancer participated in this study, whose characteristics are listed in Table 2. As is seen, mean age of the participants is 44.25. Breast cancer had been diagnosed in all the participants by oncologist specialist and they had received specialized treatment over the past years. Of the patients, only one of them has a history of receiving psychotherapy and medication. In terms of education, two of them have diploma, one is undergraduate, and the other one has a bachelor's degree. Also, regarding the job, there are two housewives, one accountant and one seller.
|
Table 2. Demographic characteristics of women with breast cancer |
||||
|
Patient 4 |
Patient 3 |
Patient 2 |
Patient 1 |
Variable |
|
45 Years |
53 Years |
38 Years |
41 Years |
Age |
|
4 Years |
6 Years |
2 Years |
3 Years |
Years of Suffering |
|
No |
Yes |
No |
No |
History of Psychotherapy |
|
No |
Yes |
No |
No |
History of Using Psychiatric Drugs |
|
Diploma |
Diploma |
Bachelor |
Undergraduate |
Education |
|
Seller |
Housewife |
Accountant |
Housewife |
Job |
According to the results presented in Table 3, the observed t level is biger than the critical the critical t (t=3.182, df=3), in death anxiety, depression, and feeling of loneliness. Thus, the mean difference of death anxiety, depression, and feeling of loneliness scores is statistically significant between the participants in the pre-test and post-test. Accordingly, it can be concluded that ISTDP has a statistically significant effect on reduced death anxiety, depression, and feeling of loneliness among women with breast cancer.
|
Table 3. Results of paired-samples t-test for comparing the mean scores of women with breast cancer in terms of death anxiety, depression, and feeling of loneliness |
|||||||||
|
Variable |
Pre-Test (Time 1) |
Post-Test (Time 2) |
Follow-Up (Time 3) |
Paired Samples T-Test |
|||||
|
|
Mean |
SD |
Mean |
SD |
Mean |
SD |
df |
T Ration (T) |
Sig |
|
Death Anxiety |
12.50 |
1.290 |
4.25 |
0.957 |
3.250 |
0.957 |
3 |
8.004 |
0.004 |
|
Depression |
12.50 |
2.081 |
3.50 |
1.29 |
2.750 |
0.957 |
3 |
12.728 |
0.001 |
|
Feeling Of Loneliness |
52.50 |
5.066 |
22.25 |
2.50 |
19.50 |
1.290 |
3 |
17.286 |
0.00 |
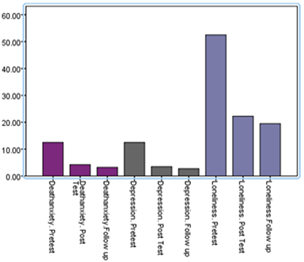
Figure 1. Comparison of pre-test, post-test and follow-up scores of the rates of death anxiety, depression and feeling of loneliness in women with breast cancer
Based on the findings of Table 4, the rates of death anxiety, depression and feeling of loneliness of women with breast cancer who participated in ISTDP program were significantly different from the pre-program rates. In this analysis, the "time" component was introduced into the model as a within- subject factor. To test the research hypothesis, a repeated measures ANOVA was used the results of which are presented in Table 4. It should be noted that before the implementation of repeated measures ANOVA, Muchley test was used to test Sphericity assumption, and the result of the test was significant (P <0.05). This means violation of this assumption. Therefore, because of the inequality of variances, the results of the Greenhouse test were considered, from among the four tests in the output of repeated measures ANOVA, in order to investigate the significance of the effect of time. The results of this table show that the effect of time on death anxiety (F=72.765, P< 0.05, ƞ= 0.960), depression (F=184.304, P< 0.05, ƞ= 0.984) and feeling of loneliness (F=202.004, P< 0.05, ƞ= 0.985) is significant.
In other words, from the pre-test session to follow-up, the rate of death anxiety, depression and feeling of loneliness in women with breast cancer has decreased significantly.
|
Table 4. The results of within-subjecs tests of difference related to the rate of death anxiety, depression and feeling of loneliness in women with breast cancer |
|
||||||
|
Effect Size |
Significance |
F value |
df of Error |
df |
Main Effect |
Variable |
|
|
0.960 |
0.003 |
72.765 |
3 |
1 |
Time |
Death Anxiety |
|
|
0.984 |
0.000 |
184.304 |
3 |
1 |
Time |
Depression |
|
|
0.985 |
0.001 |
202.004 |
3 |
1 |
Time |
Feeling Of Loneliness |
|
0.05< P
In order to more accurately compare the death anxiety, depression and feeling of loneliness scores in the pretest, post-test and follow-up, post-hoc Bonferroni test was used. According to the findings presented in table 5, there is a statistically significant difference between the rates of death anxiety, depression and feeling of loneliness of women with breast cancer in the pre-test and post-test. Thus, it can be concluded that ISTDP has been significantly effective on reduced death anxiety, depression and feeling of loneliness.
|
Table 5. Results of post-hoc Bonferroni test for comparing death anxiety, depression and feeling of loneliness in women with breast cancer |
|||||
|
Sig |
S. Error |
Mean Difference (I-J) |
Time J |
Time I |
Variable |
|
0.012 |
1.031 |
8.250 |
Post-test |
Pre-test |
death anxiety |
|
0.009 |
1.031 |
9.250 |
Follow-up |
|
|
|
0.000 |
0.000 |
1 |
Follow-up |
Post-test |
|
|
0.003 |
0.707 |
9 |
Post-test |
Pre-test |
Depression |
|
0.002 |
0.629 |
9.750 |
Follow-up |
|
|
|
0.173 |
0.250 |
0.750 |
Follow-up |
Post-test |
|
|
0.001 |
1.750 |
30.250 |
Post-test |
Pre-test |
feeling of loneliness |
|
0.003 |
2.483 |
33 |
Follow-up |
|
|
|
0.146 |
0.854 |
2.750 |
Follow-up |
Post-test |
|
Discussion
Today, diseases known as specific diseases are an inseparable part of the society in which we live. These diseases, in addition to physical problems and injuries to the patient, affect a wide range of psychological and emotional aspects of patients, which directly affect the course of the disease. It is very important to recognize and investigate the psychological components that change in these diseases and affect the mental aspect of the patient's life, because the patient continues to live in any situation under any circumstances, and the patient must try to slow down the progression of the disease as far as possible, which involves a strong spirit. One of the diseases that causes profound emotional problems in the patient and his family is breast cancer. Studies have shown that these patients are exposed to severe psychological stress that can cause psychological and social problems in their lives. A large number of people with breast cancer, due to their lack of adaptation to their illness, suffer from psychological problems and feel frustrated in their family life. The suffering and pain from the disease, the concern for the future of family members, the fear of death, the complications of treatment of disease, reduced daily functioning, mental imagination impairment and sexual problems are among the factors that disrupt the mental health of the patient with breast cancer [33].
Researchers now believe that the level of depression, anxiety and quality of life of people with breast cancer affects the lives and trends of the disease in these patients [34]. The purpose of this study was to investigate the effectiveness of ISTDP on reduced death anxiety, depression and feeling of loneliness in people with breast cancer. Statistical results showed that this approach significantly affects these components, so that the scores of the participants were lower in the post-test than in the pre-test. So, as expected, ISTDP could have a positive impact on the improvement of damaged components in these patients. In sum, few studies have been done in the world on the impact of this emerging therapeutic approach on the psychological components of these patients. However, the findings of this study are consistent with the results of previous studies, including Abbass [35]; Berger et al. [34]; Pennebaker [36]; Cramer [37]; Gross and John [38]; Stanton et al. [39]; Derogatis, Abeloff and Melisarato [40]; Weinberger [41]; Cramp [42]; Zwerenz et al. [43]; and Firestone and Catlett [44]. In explaining the findings of this study, it can be argued that depression and anxiety are the most common psychological problems of cancer patients, which is usually a reaction to the lack of apparent beauty, energy, sexual ability, freedom, and life expectancy. It is clear that depression and anxiety disorders impose a significant psychosocial stress on patients and their families, which leads to a decrease in their quality of life. Taking antidepressants and anti-anxiety drugs can cause unpleasant side effects, some of which will last until the end of life; fatigue and drowsiness, especially in the first weeks of drug use, are common side effects. Also, because cancer patients suppress their feelings of illness, become more and more alien to their own existence, and are less likely to experience new things in their minds. Consequently, they create pessimism, hatred of life, hopelessness, feeling of loneliness, and fear of death. These patients conceive of life as an unpleasant process, and the psychological system chooses to avoid it (avoiding seeing, thinking and touching the feelings of cancer). Often, these unconscious efforts fail to avoid the emotional pain of cancer, which is repeated because it is unconcious. This new therapeutic approach helps the patient re-formulate what he experiences in the treatment process more fully and tolerate the resulting discomfort. The insight from this therapeutic process increases the capacity of the patient to tolerate the emotional pain caused by the disease and raises his/her ability to think about his/her experiences and it makes the patient visualize the death and focus on his/her feelings about it, and look at life with new thoughts and a more positive view.
Conclusion
The results of this study showed that ISTDP significantly affects reduced death anxiety, depression and feeling of loneliness in people with breast cancer. Improving the components such as depression and death anxiety that affect most of the patient's life will improve the daily performance of individuals and thus improve the quality of life of these patients. In fact, this therapeutic approach, by neutralizing defenses and transitional resistance, regulating anxiety, experiencing buried feelings, and dissolving intra-psychological conflicts, causes patients to have a more positive view of their illness, experience and touch defenses, feel themselves near the other members of society and communicate with other people, instead of avoiding feelings and resorting to the defenses; this increases the life expectancy and thus reduces depression and anxiety. After interventions, the individual’s self-confidence increases and the patient feels empowered and this leads to a sense of usefulness in his/her personal life and in relation to his/her family, a good performance in daily activities and increased quality of life. As a result, attempts to create desirable mental conditions in patients with breast cancer can alter their lifestyle and improve their quality of life. Improving the level of life and the mental components in these patients can greatly improve the treatment in them. Therefore, the new ISTDP approach can be a guide for planners and authorities and used in health centers to reduce the mental disorders of people with cancer.
Acknowledgement
Thanks to all the patients and those who helped us with patience during this study.
References
- Jemal, A., Bray, F., Center, M. M., Ferlay, J., Ward, E., Forman, D. Global cancer statistics. CA: a cancer journal for clinicians, 2011; 61(2), 69-90.
- Khosravi A, Aghamohamadi S, Kazemi E, Pour Malek F, Shariati M. Mortality Profile in Iran (29 Provinces) over the Years 2006 to 2010. Tehran: Ministry of Health and Medical Education; 2013. 9: 111-116.
- Mousavi SM, Montazeri A, Mohagheghi MA, Mousavi Jarrahi A, Harirchi I, Najafi M, Ebrahimi M. Breast cancer in Iran: Anepi Demiological Review. Breast J. 2007; 13: 383-91.
- So, W. K., Marsh, G., Ling, W. M., Leung, F. Y., Lo, J. C., Yeung, M., Li, G. K. Anxiety, depression and quality of life among Chinese breast cancer patients during adjuvant therapy. European Journal of Oncology Nursing, 2010; 14(1), 17-22.
- Spiegel, D., Riba, M. B. Managing Anxiety and Depression during Treatment. The breast journal, 2015;b21(1), 97-103.
- Howard-Anderson, J., Ganz, P. A., Bower, J. E., Stanton, A. L. Quality of life, fertility concerns, and behavioral health outcomes in younger breast cancer survivors: a systematic review. Journal of the National Cancer Institute. 2012; 104(5): 1-20.
- Love S. Tehran: Noredanesh; Cases, diagnosis and prevention from breast cancer. Translatde by Taraneh Nazari; 1998; p.183.
- Degi, CL. Non-disclosure of cancer diagnosis: an examination of personal, medical, and psychosocial factors. Support Care Cancer, 2009; 17(8): 1101-7.
- Fu, MR., Xu, B., Liu, Y., Haber, J. 'Making the best of it': Chinese women's experiences of adjusting to breast cancer diagnosis and treatment. J Adv Nurs, 2008; 63(2): 155-65.
- Belsky, g. The psychology of aging. Brooks / cole publishing company: 1999; P 368.
- Naderi, F., Seyyedeh Hosseini, M. Relationship between life expectancy and psychological hardiness in male and female students of Islamic Azad University of Gachsaran. Women and Society Quarterly, 2010; 1 (2):123-137.
- Jones, H.E., Simon, L., Greenberg, J., Pyszczynski, T., Solomon, S., McGregor, H. Terror management theory and selfesteem: Evidence that increased self Esteem reduced mortality salience effects. J Pers Soc Psychol 1997; 72(1):24.
- Karakoyun-Celik, O., Gorken, I., Sahin, S., Orcin, E., Alanyali, H., Kinay, M. Depression and anxiety levels in woman under follow-up for breast cancer: relationship to coping with cancer and quality of life. Medical Oncology, 2010; 27(1), 108-1
- Trief, PM., Donhue, M. Counseling needs of women with breast cancer. Psychosicuak byrsubg, 1996; 34 (5): 24 –29.
- Fukui, S., Koike, M., Ooba, A., Uchitomi, Y. The effect of a psychosocial group interventionon loneliness and social support for Japanese women with primary breast cancer. Oncol Nurs Forum, 2003; 30(5):823–30.
- Weiss, RS. Reflections on the present state of loneliness research. J Soc Behav Pers. 1987; 2: 1-
- Hojat, M. Comparison of transitory and chronic loners on selected personality variables. Brit J Psychol. 1983; 74: 199-202.
- Wells, M., Kelly, D. The loneliness of cancer. Euro J Oncol Nurs, 2008; 12(5): 410-1.
- Saklofske, DH., Yackulic, RA. Personality predictors of loneliness. Pers Indiv Diff. 1989; 10: 467-72.
- Ernst, J., Cacioppo, J. Lonely hearts: Psychological perspectives on loneliness. Appl Prev Psychol. 1999; 8: 1-22.
- Ditommasso, E., Brannen, C., Best, LA. Measurement and validity characteristics of the short version of the social and emotional loneliness scale for adults. Edu Psychol Meas. 2004; 64(1): 99-119.
- Ghorbani, N. Intensive short-term dynamic psycho-therapy. Tehran: SAMT publications, 2013.
- Davanloo, H. Unlocking the unconscious. (A. Sigadri Khalighi, Trans.) Tehran: Arjomand publications, 2016.
- Malan, D.H. The most important development in psychotherapy since the discovery of the unconscious. In: H. Davanloo (Ed.), Short –Term Dynamic Psychotherapy (pp. 13-23). New York: Aronson, 1980.
- Jarareh, J. Comparison of the effectiveness of intensive short-term dynamic psycho-therapy and Setir communicative approach in increasing the satisfaction of couples. Doctoral dissertation, Faculty of Psychology and Educational Sciences, Allameh Tabatabaei University, 2007.
- Wolf, D. Frederickson, J. Intensive short-term dynamic psychotherapy. Washington School of Psychiatry, Retrieved April 8, 2012. From: www.davidwolffmd.com
- Driessen, E., Hegelmaier, L.M., Abbass, A.A., Et Al. The Efficacy of Short - Term Psychodynamic Psychotherapy for Depression: A Meta- Analysis Update. Clinical Psychology Review, 2015; 42, 1-15
- Templer, D. I. The construction and validation of a death anxiety scahe. The gournal of general psychology, 1970; 82, 165-177.
- Rajabi, Gh., Bohrani, M. Factorial analysis of death anxiety scale. Psychol J, 2001; 4: 331-44.
- Rajabi, Gh.R. Psychometric properties of short-form items of Beck Depression Inventory (BDI-13), Shahid Chamran University, 2005.
- Lightfood, SL., Olliver, JM. The Beck Inventory: Psychometric Properties in university students. Journal of Personality Assessment, 1985; 49 (4), 434- 436.
- Mahdavi, A., Taghizadeh, M.A., Esazadeh, S., Salehi, S., Darabi, R., Rafigh, P. Relationship Between Depression and Perceived Stress with Marital Satisfaction in Individuals Suffering Cancer and Cardiovascular Diseases. Advances in Natural and Applied Sciences, 2015; 9(2): 50-58.
- So, W. K., Marsh, G., Ling, W. M., Leung, F. Y., Lo, J. C., Yeung, M., Li, G. K. The symptom cluster of fatigue, pain, anxiety, and depression and the effect on the quality of life of women receiving treatment for breast cancer: a multicenter study. In Oncology nursing forum. 2009; 36(4), E205- E214.
- Berger, A. M., Wielgus, K., Hertzog, M., Fischer, P., Farr, L. Patterns of circadian activity rhythms and their relationships with fatigue and anxiety/depression in women treated with breast cancer adjuvant chemotherapy. Supportive care in cancer, 2010; 18(1), 105-114.
- Abbass, A. Intensive short term dynamic psychotherapy in private psychiatric office: clinical and cost effectiveness. American journal of psychotherapy, 2002a; 56: 225-232.
- Pennebaker, J.W. Opening Up: The healing power of confiding in others. New York: Morrow, 1991.
- Cramer, P. Defense mechanisms in psychology today: Further processes for adaptation. American Psychologist, 2000; 55: 637-646.
- Gross, J.J., John, O.P. Revealing feelings: Facets of emotional expressivity in self – reports, peer ratings, and behavior. Journal of personality and social psychology, 1997; 72: 435-448.
- Stanton, A.L., Danoff-Burg, S., Cameron, C.L., Bishop, M., Collins, C.A., Kirk, S.B., Sworowski, L.A. Emotionally expressive coping predicts psychological and physical adjustment to breast cancer. Journal of Consulting and Clinical Psychology, 2000; 68: 875-882.
- Derogatis, L.R., Abeloff, M.D., Melisarato, S.N. Psychological coping mechanisms and survival time in metastatic breast cancer. Journal of the American medical association, 1997; 242: 1504- 1508.
- Cramp, F., Daniel, J., Exercise for the management of cancer-related fatigue in adults. Cochrane Database of Systematic Reviews, 2008; 2.
- Weinberger, D.A. The construct validity of the repressive coping style. In J. L. Singer (Ed.), Repression and Dissociation: Implications for Personality Theory, Psychopathology, and Health (pp. 337-386). Chicago, IL: University of Chicago Press, 1990.
- Zwerenz et al. Efficacy of psychodynamic short-term psychotherapy for depressed breast cancer patients: study protocol for a randomized controlled trial. BMC Cancer, 2012. https://doi.org/10.1186/1471-2407-12-578.
- Firestone R, Catlett. Beyond death anxiety. New York: Springer Publishing Company 2009.
Contact SPER Publications
SPER Publications and
Solutions Pvt. Ltd.
HD - 236,
Near The Shri Ram Millenium School,
Sector 135,
Noida-Greater Noida Expressway,
Noida-201301 [Delhi-NCR] India