
Unilateral variations in divisions of left common Carotid Artery – a case report
Ardeshir Moayeri1, Azim Hedayatpour2, Marzieh Darvishi1*, Alireza Afifipour1, Pooyan Kamalivand1
1 Department of Anatomy, Faculty of Medicine, Ilam University of Medical Sciences, Ilam, Iran. 2 Department of Anatomical Sciences, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
Correspondence: Marzieh Darvishi, Department of Anatomy, Faculty of Medicine, Ilam University of Medical Sciences, Ilam, Iran. E-mail: [email protected]
|
ABSTRACT A variation of the right common carotid artery (CCA) was found after routine dissection of a 28-year-old male cadaver. on right side, carotid arose from the brachiocephalic trunk behind the sternoclavicular joint, and the bifurcation of CCA to external and internal carotid artery normally occurs 1cm just above the lamina of thyroid cartilage. While onthe left side, carotid artery arose from the aortic arch and divided in face, above and behind the angle of the mandible on 4cm higher than the superior lamina of thyroid cartilage. The arteries did not have any branches on the cervical region on the left side, after bifurcation of CCA; external carotid branch passes 4.5 cm and then divides into two branches. One of the branches is a facial artery which crosses the inferior border of the mandible, and it enters the face between the submandibular gland and mandible. The precise location of the CCA bifurcation is of great necessity in head and neck surgeries in order to prevent rupture and hemorrhage. A high CCA bifurcation increases the risk of arterial rupture in therapeutic procedures such as thyroid and parathyroid surgeries, ENT interventions and radiological examinations. Keywords: common carotid bifurcation, external carotid artery, internal carotid artery, anatomical variation |
Introduction
Division of CCA and orientation of external carotid artery (ECA) branches are essential for diagnosis and surgical procedure in neck. The origin of the CCA is different on both sides [1]. CCA is a branch of the brachiocephalic trunk on the right side and arch of the aorta on the left side which arises adjacent to the posterior part of the sternoclavicular joint [2]. It divides into the external and internal carotid artery on the superior border of thyroid cartilage, at the level of intervertebral disc of C3 and C4 cervical vertebrae [3]. The ECA supplies the facial structures, exterior region of the scalp, greater part of neck and superior pole of thyroid while, internal carotid artery (ICA) supplies the cranial and orbital cavities [4]. The cervical portions of the CCA resemble each other in a way that, each vessel ascends the sternoclavicular joint posteriorly to the level of the intervertebral disc of C3 and C4, where it bifurcates. The CCAs are separated from each other by the trachea and thyroid gland, larynx and pharynx. At the site of bifurcation, the ICA usually takes a deeper path and is posterolateral to the ECA that gives off no branches in the cervical region, whereas the external does. This study reports unilateral variations in the bifurcation of CCA [5].
Case Report
This case is reported for unusual division of CCA and branching pattern of ECA on the left side of the cadaver. During dissection of the left and right CCAs, in the Department of Anatomy, Ilam University of Medical Sciences, we found unilateral variation on the bifurcation of CCA in a 28-year-old male cadaver. The dissection of the cadaver was carried out according to the Cunningham’s manual of practical anatomy after fixation with 4% formalin. The skin was exposed from the chin to the suprasternal notch. On both sides the CCA was then exposed as were the branches of the ECA. The rCCA arose from the brachiocephalic trunk in proximity of the sternoclavicular joint as was expected and then it crossed the neck and ascended along its course within the carotid sheath where the internal jugular vein and vagus nerve is located lateral and posterior to it, respectively (fig1).
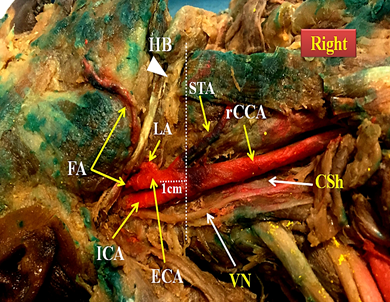
Figure 1: Figure showing right common carotid artery and its related structures. (rCCA: right common carotid artery; ECA: external carotid artery; ICA: internal carotid artery; STA: Superior thyroid artery; LA: lingual artery; HB: hyoid bone; FA: facial artery; CSh: carotid sheath; VN: right vagus nerve)
On right side, the level of division of CCA was correlated with 1cm from the superior margin of thyroid cartilage. After bifurcation, the right superior thyroid artery arose from the anterior surface of ECA and passed the superior border of thyroid gland directly. The right facial artery and lingual artery arose from the anterior of ECA just lower and above the angle of the mandible, respectively. The right facial artery coursed along the posterior border of the mandibular ramus and superficial portion of submandibular gland, and then gave off muscular branches to facial muscles.
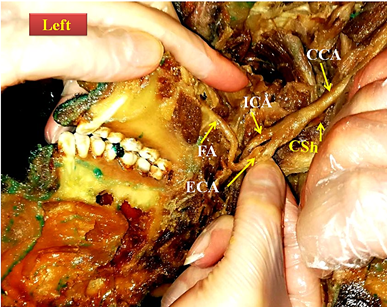
Figure 2: Figure showing left common carotid artery and its related structures (before staining). (CCA: Common carotid artery; ECA: external carotid artery; ICA: internal carotid artery; FA: facial artery; SC: Carotid sheathe
The left CCA (lCCA) originated from the arch of the aorta, subsequently passes through the posterior part of the sternoclavicular joint. After entering the neck, the artery lied within the medial part of the carotid sheath. The rCCA and lCCA gave off no branches proximal to their divisions. In the present study, unilateral variation in the bifurcation levels of lCCA was detected. The bifurcation of the lCCA was at the levels of the upper and behind of the angle of the mandible and 4cm upper to thyroid cartilage. The left ECA approximately 2 cm above the level of bifurcation is divided into two arteries, first branch is the facial artery that has variation on its origin and course. The second branch ascends to the infra temporal fossa and divides into maxillary and superficial temporal arteries. On the left side the superior thyroid, lingual, occipital and posterior auricular arteries were absent. These branches were normal on the right side.
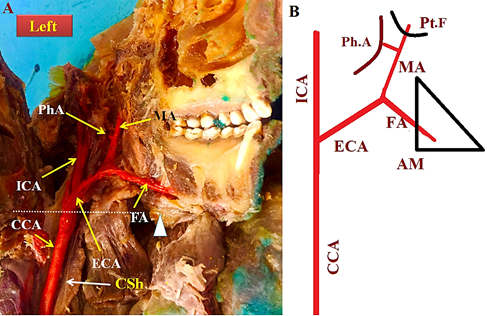
Figure 3: A, Figure showing left common carotid artery and its related structures (after staining). (CCA: Common carotid artery; ECA: external carotid artery; ICA: internal carotid artery; phA: pharyngeal artery; FA: Facial artery; CSh: Carotid sheath; MA: maxillary artery; Pt.F: pterygoid fossa; Ph: pharynx). The triangle shows the angle of mandible. B, the schematic figure of left common carotid artery and its related structures.
Discussion
The ventral segment and aortic sac opposite the 3rd arch is the fetal origin of CCA. The dorsal portion of the 3rd arch artery and the dorsal segment of the aortic arch form ICA. The ECA is also derived from the sprouts of the aortic sac adjacent of the ventral segment of the third arch. The outgrowth of the sprout from a higher point leads to the division of the artery in the higher level [6]. The unilateral and bilateral variation in the bifurcation of CCA is not common; Patil et al. (2012) showed variation of bifurcation of CCA on the right side 4.2 cm and on left side 3.5 cm just behind the angle of the mandible and at the higher level [1]. In another case report Deshpande et al. (2015) showed that multiple variations in the CCA bifurcation level, tortuous ICA and ECA and the number of branches arising from ECA. The state of arrangement of an artery in the face may lead to loop formation outside of the pharyngeal wall which is known as the “dangerous loop.” These variations are pivotal for surgeons and radiologists in case of cutaneous carotid angiography [7]. If the CCA bifurcation occurs at a higher level in that case, the hypoglossal nerve will be in relation to the CCA. Smith and Larsen (1979) reported that the CCA bifurcation at higher than normal levels, occurs more commonly on the left side [8]. These findings are in agreement with this case report. In the present case we found unilateral higher division of lCCA, and the absent of the left superior thyroid artery and lingual artery. The anatomic consequences of such variations of the CCA birfurcation have been one of the risks of rupture of the artery during the vascular surgical procedures for carotid endoplasty, extracranial–intracranial arterial bypass, ear and throat surgeries that lead to surgical complications [9]; hence, surgeons and radiologists should be aware of these types of variations to prevent the rupture or bleeding caused by damage to the artery in an unusual position. A high CCA bifurcation is at a higher risk of encroachment by intra-articular torsion during procedures on the neck and face, and they are associated with higher occurrence of vascular rupture [10].
Abbreviations
CCA, common carotid artery; ECA, external carotid artery; ICA, internal carotid artery; rCCA, right common carotid artery; lCCA, left common carotid artery.
References
- Patil BS, Desai SD, Bagoji IB, Hadimani GA. Bilateral variations in the divisions of common carotid artery–a case report. Int J Anat Var (IJAV). 2012;5:116-9.
- Standring S. The anatomical basis of clinical practice 40th Edition. Philadelphia: Elseveir Churchill Livingston. 2008:978-80.
- Adams GJ, Simoni DM, Bordelon Jr CB, Vick III GW, Kimball KT, Insull Jr W, Morrisett JD. Bilateral symmetry of human carotid artery atherosclerosis. Stroke. 2002 Nov 1;33(11):2575-80.
- Avadhani R, Chakravarthi KK. Multiple bilateral anomalies of carotid arteries-a case report. Nitte University Journal of Health Science. 2012 Sep 1;2(3).
- Bergman RA, Thompson SA, Afifi AK. Compendium of man Anatomical variation: Catalog, Atlas and World literature. Baltimore and Munich: Urban & Schwarzenberg. 1998;64.
- Moore K., Dalley A., Agur, A. Anterior cervical region: Clinically oriented Anatomy. 6thed. Lippincott Williams &Wilkins, Philadelphia, 2010; 998-1012.
- Deshpande SH, Nuchhi AB, Bannur BM, Pital B.Bilateral Multiple Variations in Carotid Arteries-A Case Report. J Clin Diagn Res. 2015; 9(12): AD01–AD03.
- Radha K. Bifurcation levels of the common carotid arteries: a cadaveric study in south Indian population. Int J Anat Res. 2014;2(3):511-14.
- Smith D, Larsen JL. On the symmetry and asymmetry of the bifurcation of the common carotid artery. Neuroradiology. 1979 Jan 1;17(5):245-7.
- Hayashi N, Hori E, Ohtani Y, Ohtani O, Kuwayama N, Endo S. Surgical anatomy of the cervical carotid artery for carotid endarterectomy. Neurologia medico-chirurgica. 2005;45(1):25-30.
Contact SPER Publications
SPER Publications and
Solutions Pvt. Ltd.
HD - 236,
Near The Shri Ram Millenium School,
Sector 135,
Noida-Greater Noida Expressway,
Noida-201301 [Delhi-NCR] India